
Oct 29, 2018
This article was provided by World Stroke Organisation
Today on World Stroke Day, October 29th the World Stroke Organization, is calling for urgent action and investment to address the growing burden of stroke and circulatory diseases globally.

Prof Michail Brainin
Photo credit WSO
Highlighting the disappointing outcome of the recent UN High Level Meeting on Non-Communicable Diseases (NCDs) the WSO President, Prof Michael Brainin said, ‘We know that we 80% of strokes could be prevented by addressing a small number of risk factors, including hypertension, diet, smoking and lack of exercise. We also know that action on prevention would also contribute to a massive scale reduction in heart disease, cancer and diabetes.’
‘The impact of stroke on individuals, families and society as a whole is devastating. Stroke survivors can face significant impairment of movement, speech, cognition alongside debilitating psychological, social and financial problems.
‘With this knowledge, the current lack of political will and investment is cannot be easily comprehended, especially when you consider the cost of such inaction. While 5.5 million people die as a result of stroke each year, there are 80m stroke survivors in the world, many of whom live with some form of disability or impairment. While the costs to individuals is incalculable, the cost to society is astronomical.’
A recent policy document ‘Driving Sustainable Action for Circulatory Health’ published by the WSO and its partners in the Global Coalition for Circulatory Health, has calculated the global cost of circulatory diseases, including stroke, at US$957 Billion in 2015. On current projections this figure is set to rise to US$1044 Billion by 2030. The white paper sets out four key areas for action that, if enacted, would ensure delivery of global goals on disease reduction which are driving the rise in direct and indirect costs of NCDs. These include legislative interventions that:
1. Deliver policies and programmes to address tobacco, alcohol and unhealthy foods, promote clean air and deliver a built environment that fosters safe physical activity.
2. Ensure access to affordable, quality-assured essential medicines, delivered by adequately trained staff, including access to multi-therapy treatments.
3. Mobilise sufficient resources to combat non-communicable diseases including stroke. The taxation of unhealthy products such as alcohol, tobacco, unhealthy foods and non-alcoholic beverages (such as sugar-sweetened beverages) would generate revenues that could be directed to further prevention and control of circulatory diseases at global and national levels.
4. Put in place reliable, simple, and fit-for- purpose surveillance systems for monitoring the burden of stroke and the prevalence of NCD risk factors and treatment of stroke at national and global levels.
Prof Brainin concluded ‘At the recent UN High Level Meeting on NCDs in New York, governments delivered a weak response to a global crisis and agreed to wait 7 years before reviewing progress. In that time another 38.5 million people will die of stroke. We can’t wait until 2025 to calculate our losses, we need strong leadership and bold action to save lives now.’

Oct 29, 2018
Today is World Stroke Day, October 29th. Though stroke may feel isolating, there are millions of survivors in the world. Stroke recovery is a community effort, and there needs to be a more clearly defined pathway from prevention to rehabilitation.
 Taking that into account, SAFE is proud to announce the publishing of the Stroke Action Plan for Europe 2018-2030. This document is a result of collaborative work between SAFE and European Stroke Organisation (ESO), being an intersection and a point of confluence for large experiences coming from SAFE’s members, stroke survivors and patient advocates from one side and medical experts, specialised in stroke and stroke related research.
Taking that into account, SAFE is proud to announce the publishing of the Stroke Action Plan for Europe 2018-2030. This document is a result of collaborative work between SAFE and European Stroke Organisation (ESO), being an intersection and a point of confluence for large experiences coming from SAFE’s members, stroke survivors and patient advocates from one side and medical experts, specialised in stroke and stroke related research.
“With this great collaboration we are trying to make sure more attention is paid to the whole stroke care pathway. Fatigue, long-term pain, finance, work or unemployment, relationships, aphasia- these things are usually not in front of mind for many medics or politicians and healthcare decision makers. Therefore, the addition of Life After Stroke domain as one of the Stroke Action Plan’s priorities is an important step forward. SAFE is working with ESO to ensure that we jointly engage with politicians and decision makers until the whole action plan is being implemented” said Jon Barrick, SAFE President.
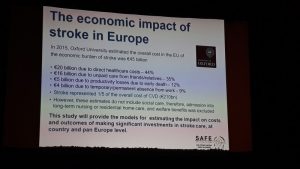
This year, around 610,000 people in the European Union will have a stroke, and, although the figures are patchy, at least 170,000 people in non-EU European countries will have one. That is more than one stroke a minute. Their stroke could be devastating – leading to death or life-long disability, shattering their lives and those of their loved ones. Those who survive their stroke will join the millions of stroke survivors across Europe who live with the health, social and financial impacts.
“Long term commitment and attention to the needs and rights of stroke survivors and their caregivers will contribute to better health and wellbeing, outcomes, increase independence and reduce demand on healthcare, social and welfare systems” concluded Barrick.
The popular version of the Stroke Action Plan for Europe 2018-2030 can now be downloaded from HERE.
The scientific version of this document is also available starting from today and can be downloaded from the following LINK.

Oct 26, 2018
On Monday, October 29th stroke support organisations from around the world will create a global moment to demonstrate that there is life after stroke – that a stroke may bring you down but that it’s possible to get #UpAgainAfterStroke.
It is estimated that there are around 80 million stroke survivors around the world each one facing many challenges of daily living after having had a stroke. Stroke survivors face many obstacles and the scale of this is dependent on where they live, their socioeconomic status and the severity of their stroke.
Despite these obstacles on World Stroke Day 2018 we want to focus the world’s attention on what unites stroke survivors and caregivers – their resilience, their capacity to build on the things that stroke can’t take away and their determination to keep going on their journey of recovery.
 For every stroke survivor, Getting Up Again After Stroke takes commitment. Building support networks with other stroke survivors, sharing stories of survival and recovery can help people stay hopeful and focused on progressing.
For every stroke survivor, Getting Up Again After Stroke takes commitment. Building support networks with other stroke survivors, sharing stories of survival and recovery can help people stay hopeful and focused on progressing.
At the same time, caring for someone who has had a stroke can be demanding and many of the relationships that bind us change. It is understandable that carers need help too.
Policy-makers need to understand that long term commitment and attention to the needs and rights of stroke survivors and their caregivers will contribute to better health and wellbeing, outcomes, increase independence and reduce demand on healthcare, social and welfare systems.
SAFE member organisations from 30 European countries are preparing a series of events to mark World Stroke Day this year, under an overarching theme #UpAgainAfterStroke.
Find your country’s organisation HERE and help us raise stroke awareness for this World Stroke Day.
Stroke Alliance for Europe with all our members from 30 European countries, proudly stands with the stroke survivors and their families on October 29th, World Stroke Day.

Oct 24, 2018
The slogan and hashtag of this year’s World Stroke Day is #UpAgainAfterStroke. The SAFE member organisation from Serbia sent us a very inspirational story of a young woman who managed to conquer stroke and kept pursuing her dreams.

Photo: Private archive of Marina Krsmanovic
Marina Krsmanovic from Serbia, a nursery teacher and mother of two, never was a smoker and did sports on regular basis. Despite her healthy lifestyle, in December 2017 she felt that her right arm was paralysed, she lost her sight and she noticed speech difficulties.
She did not wait and she immediately called for help. Within one hour she was admitted to St. Sava (Sveti Sava) Special Hospital for cerebrovascular diseases in Belgrade, Serbia. The medics diagnosed a stroke which was a consequence of a congenital heart disease. She was sent to the Institute of Cardiovascular diseases where she had a heart surgery on 24th January 2018.
She found her motivation and strength for recovery in her children. She adopted a new diet, changed the way of thinking and she now says that she has started enjoying her life, finding happiness in small things and that she always has positive thoughts. It’s safe to say that her fast reaction at the first symptoms, quick transportation to hospital and of course high quality treatment in the above mentioned medical institutions were the key for her successful recovery. Now, she can function independently, she has returned to her workplace…
When we got in touch with her, we heard some great news and it’s not enough to say that we were amazed. Apart from returning to her everyday routine, Marina has returned to her hobby that she practiced before stroke- downhill mountain biking. She even won a medal at a competition that took place on Zlatibor mountain (Western Serbia) at which she was the only female competitor!

Photo: Private archive
She said that her only goal has been to take part in the competition and to prove it to herself that she could tame the mountain once again. Taking part in the competition is worth all the attention and admiration one could get but winning a medal is like reaching the top of the world.

Photo: Private archive
Her message to all of us is stick to positive thinking, enjoy little things and enjoy your life to the fullest. We hope that Marina’s story will motivate people never to give up and to keep fighting. We, on our behalf, have a duty to do everything we can to make life easier for those who had suffered a stroke, to help them get #UpAgainAfterStroke!
If you want to share your experiences with SAFE and if you want set an example for people who are facing a stroke and all its consequences, please contact us via Facebook and Twitter.

Oct 21, 2018
At this year’s World Stroke Congress In Montreal, Canada, SAFE was present through a variety of activities, from chairing stroke support sessions, being one of the key speakers and presenters, having a very well noticed and visited information stand, to actively participating in the World Stroke Day workshop and shaping the World Stroke Campaign in the years to come.
SAFE President Jon Barrick presented the SSOFT project, an online ‘how to’ toolkit for a range of advocating skills training, from setting up a stroke support organisation to leading PR and advocacy campaigns. This tool aims to build capacity of the European SSOs but can be used much broader to increase one world voice for stroke. His presentation sparked interest even among SSOs from other continents leading to an interesting exchange of ideas and suggestions for its further development. The SSOFT project will be completed by end of November 2018. Project team are looking at the future development such as translation into other languages, additional modules, global scope, said Barrick, but it is depending on funding. The presentation was broadcasted live on Facebook and the video can be found here.
In addition to the SSOFT project, SAFE had a chance to present the economic Burden of Stroke Report, scheduled to be published towards the end of 2019, as well as the SAFE & Industry Partner collaboration project on Life With Spasticity.
 However, the Stroke Action Plan for Europe 2018-2030, a joint SAFE and ESO project got the majority of attention due to the fact that it just has been launched in May this year and is aimed to set the road map for stroke prevention, treatment and life after stroke in Europe in the next 12 years.
However, the Stroke Action Plan for Europe 2018-2030, a joint SAFE and ESO project got the majority of attention due to the fact that it just has been launched in May this year and is aimed to set the road map for stroke prevention, treatment and life after stroke in Europe in the next 12 years.
Successful examples and case studies from around the world, such as the one of the Swedish Stroke Registry and their latest project about caregivers and how they are coping with the consequences of strokes in their loved ones. The need for comprehensive and systematic follow up reviews for stroke survivors, after 3, 6 and 12 months was particularly stressed out.

Prof. Bo Norrving
We heard from Prof. Bo Norrving, University of Lund, Sweden, that one of 6 strokes was eradicated in Sweden over the last 6 years, meaning 14,000 in absolute number of strokes, and saving one billion euros. The reason for this success lays in treatment of TIA, atrial fibrillation and use of preventive medications. Stroke is probably the single most preventable disease of all. It may be that I am wrong, but I would like to be proven to be wrong, said Prof. Norrving.
During a separate open session on stroke as part of the non-communicable disease, Stephanie Mohl on behalf of American Heart and Stroke Association opened the conversation saying: Here we are in 2018 and we still need to talk about why patients need to in center of the healthcare, pointing towards all of the necessary efforts to convince the policy decision makers to listen to the patient voice in almost all parts of the world.
The way non-communicable diseases were addressed so far by the policy makers, the NCD acronym might as well stand for No Can Do, said Jon Barrick. This needs to be changed, but we need to be aware that people don’t put energy into hopeless campaigns, so stroke support organisations should be more active in showing perspectives and opportunities for stroke survivors and their carers.
SAFE was active on social media during the whole three days of the World Stroke Congress. For more information, please visit our social media accounts on Facebook and Twitter.

An open session on stroke and non-communicable diseases


